


AK is a premalignant lesion of the skin caused by chronic sun damage.1,2,4
AKs may:
Be easier felt than seen and can appear rough or scaly5
Range in color from normal skin tone to reddish brown1
Be tender or itchy and may bleed6,7
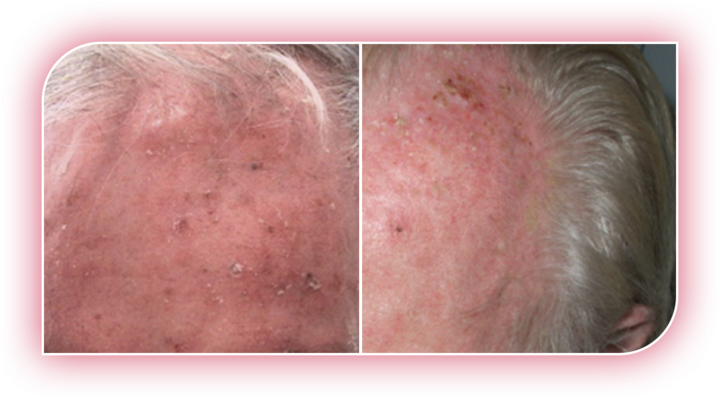
AK lesions on the face and scalp
Because AKs originate in the skin layers below the visible surface, lesions can be present but still difficult to spot. For every visible lesion within a sun-damaged area, there are likely other AKs that are easier felt than seen. Together, these lesions are considered a field.2,3,8

AKs can affect anyone, but they are most common in people4,9:
Since we cannot tell which AK lesions will develop into skin cancer, it is recommended to treat your AKs.10,11
For every AK lesion you can see, there are likely more lesions that you can feel but may be difficult to see.3,5



If you have any questions about AMELUZ®, please contact your health care provider.
For every AK lesion you can see, there are likely more lesions that you can feel but may be difficult to see.3,5

If you have any questions about AMELUZ®, please contact your health care provider.
For every AK lesion you can see, there are likely more lesions that you can feel but may be difficult to see.3,5

If you have any questions about AMELUZ®, please contact your health care provider.
INDICATION
AMELUZ® (aminolevulinic acid hydrochloride) topical gel, 10%, a porphyrin precursor, in combination with photodynamic therapy using BF-RhodoLED®a lamp, is used for lesion-directed and field-directed treatment of actinic keratoses (AK) of mild-to-moderate severity on the face and scalp.
IMPORTANT SAFETY INFORMATION
Purpose: Photosensitizing agent
Uses: AMELUZ®, a porphyrin precursor, in combination with photodynamic therapy using BF-RhodoLED®a lamp, is used for lesion-directed and field-directed treatment of actinic keratoses (AK) of mild-to-moderate severity on the face and scalp.
Warnings:
Do not use if you have a:
Ask your health care provider before use if you have:
When using this product:
Most common side effects at the application site were:
Most side effects occurred during illumination or shortly afterwards, were generally of mild or moderate intensity, and lasted for 1 to 4 days in most cases; in some cases they persisted for 1 to 2 weeks or even longer.
Pregnancy Warning: There is no available data on AMELUZ® use in pregnant women to inform a drug associated risk.
Lactation Warning: There is no available data regarding the presence of the active ingredient (aminolevulinic acid hydrochloride) in human milk, or the effects of aminolevulinic acid hydrochloride on the breastfed infant or on milk production.
Pediatric Warning: Safety and effectiveness in pediatric patients below the age of 18 has not been established.
Geriatric Warning: No overall differences in safety or effectiveness were observed between older (65 years and older) and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Directions:
Inactive Ingredients: xanthan gum, soybean phosphatidylcholine, polysorbate 80, medium-chain triglycerides, isopropyl alcohol, dibasic sodium phosphate, monobasic sodium phosphate, sodium benzoate and purified water.
Other Information:
aAMELUZ® is also approved in combination with photodynamic therapy using RhodoLED® XL lamp, which is currently not available for distribution.
References: 1. Reinhold U. A review of BF-200 ALA for the photodynamic treatment of mild-to-moderate actinic keratosis. Future Oncol. 2017;13(27):2413-2428. 2. Stockfleth E. The importance of treating the field in actinic keratosis. J Eur Acad Dermatol Venereol. 2017;31(Suppl 2):8-11. 3. Berman B, Amini S, Valins W, et al. Pharmacotherapy of actinic keratosis. Expert Opin Pharmacother. 2009;10(18):3015-3031. 4. Actinic keratosis risk factors. Skin Cancer Foundation website. Updated January 2022. Accessed November 3, 2025. https://www.skincancer.org/skincancerinformation/actinic-keratosis/causes-and-risk-factors. 5. Olsen EA, Abernethy L, Kulp-Shorten C, et al. A double-blind, vehicle-controlled study evaluating masoprocol cream in the treatment of actinic keratoses on the head and neck. J Am Acad Dermatol. 1991;24:738-43. 6. Actinic keratosis. Mayo Clinic website. Updated December 17, 2022. Accessed July 11, 2023. https://www.mayoclinic.org/diseases-conditions/actinickeratosis/symptomscauses/syc-20354969. 7. Actinic keratosis: signs and symptoms. American Academy of Dermatology Association website. Updated 2023. Accessed July 8, 2023. https://www.aad.org/public/diseases/skin-cancer/actinic-keratosis-overview. 8. Cockerell CJ. Histopathology of incipient intraepidermal squamous cell carcinoma ("actinic keratosis"). J Am Acad Dermatol. 2000;42(1 Pt 2):11-7. 9. Skin cancer (non-melanoma): risk factors and prevention. Cancer.net website. Updated February 2022. Accessed July 11, 2023. https://www.cancer.net/cancer-types/skin-cancer-non-melanoma/risk-factors-and-prevention. 10. Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg. 2007;33(9):1099-101. 11. Del Rosso J, Armstrong AW, Berman B, et al. Advances and considerations in the management of actinic keratosis: an expert consensus panel report. J Drugs Dermatol. 2021;20(8):888-893. 12. Grada A, Muddasani S, Fleischer AB, et al. Trends in office visits for the five most common skin diseases in the United States. J Clin Aesthet Dermatol. 2022;15(5):E82-E86.